Why is shame a common patient emotion in conversations about dental habits?
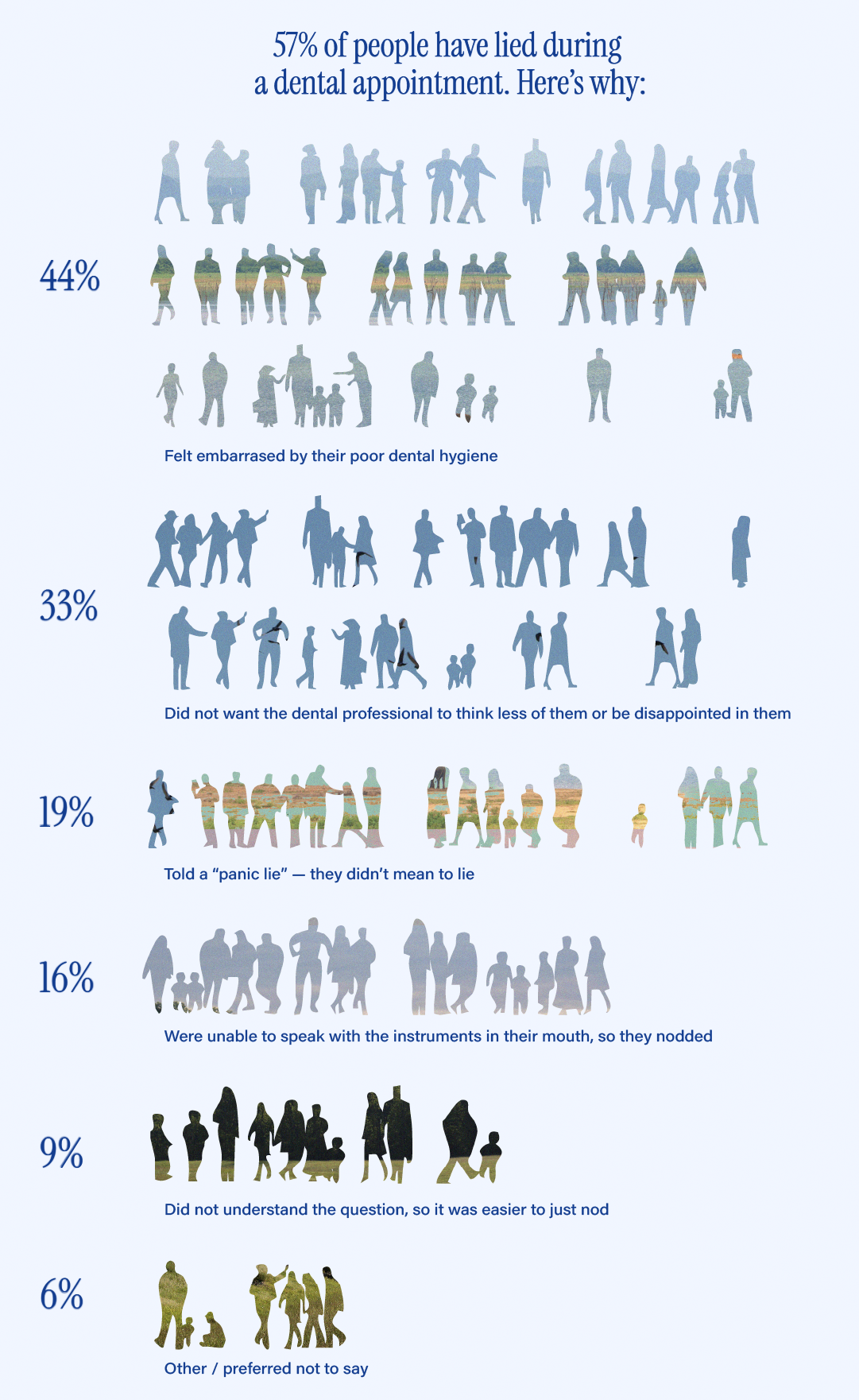
In a survey of 2000 Americans, over half of the respondents (57%) admitted to lying to their dentist about their oral care routine. 44% of them did it because they felt embarrassed by their poor dental hygiene and a further 33% wanted to avoid their dentist thinking less of them. All this highlights just how tightly oral care is associated with perceptions of “responsible behaviour”.
These emotions are reinforced by the broader societal stigmas in play: We conflate good oral health with higher social status, hence the cultural fixation on “straight, white teeth” as a marker of success and self-discipline.
Meanwhile, dental professionals spend their time engrossed in the world of oral health, constantly engaging with the effects of poor oral hygiene. This creates a desensitisation to the topic.
Giving advice on dental habits rarely comes from a place of judgment, especially when we are giving the same advice over and over. But for the patient, it may be their first time hearing it; they are unlikely to be aware of how common it is, and so their perception of the topic will be different.
“As a psychologist, when I talk to my clients about their diagnosis or treatment plan, it is a normal thing I talk about every day. But I have to be really careful to say it in a very sensitive manner because I have to remember that my clients may never have had this kind of conversation in their lives.
The same thing happens with dental professionals.”
Psychologist and anxiety expert Denisa Moravcik Debrecka
What are the effects of shame?
If the patient feels shamed by the dental professional’s comments on their oral care, they are likely to close off or otherwise attempt to protect themselves from the feeling, all of which leads them to be less receptive to the advice given. Avoidant behaviour is one of the most common responses to shame (or anticipated shame), which in a healthcare setting can include:
- Lying about health habits
- Concealing details about one’s life situation, including physical or mental health
- Avoiding appointments
- Not completing the course of prescribed treatment
This also means that if a patient has felt ashamed or embarrassed by the interaction, they are more likely to conceal or lie about their health habits next time, and they are also less likely to return.
A 2020 paper surveyed 11,382 adult individuals in the UK to test the interplay of shame, communication, trust, anxiety and the effect this has on dental attendance. They proposed the following model in which the arrows illustrate the associations of these latent variables (i.e. patient feelings of shame affects the trust they have in their dentist, the trust they have in their dentist affects their dental attendance, and so on.)
As the model shows, patient feelings of shame can be present before the appointment has even started (due to social stigmas or internalised beliefs), making it even harder to discuss oral health habits without the patient feeling judged.
Of course, this doesn’t mean the topic should be avoided entirely. It is important to be honest with patients about their oral health. So, how can we do it?
How to approach a shame-sensitive oral hygiene conversation
There is no one-size-fits-all approach to patient communication, but combining empathy with intentional language can make a world of difference. Here are some ways to approach oral hygiene conversations with care:

1. Pay attention to how you ask questions
When asking about oral health habits, avoid phrasing that sounds accusatory or implies disappointment. Even subtle shifts in wording can help prevent the patient from feeling defensive.
- Instead of: “How often are you really brushing?”
- Try: “Can you tell me about your brushing routine?”
Open questions invite honesty without implying judgment, especially when paired with a warm tone and open body language.

2. Normalise the patient’s experience
Let patients know they are not alone. Normalising the experience can diffuse shame and encourage open dialogue. Remember that oral hygiene lapses often reflect broader life challenges, so don’t hesitate to acknowledge that keeping up with a routine is not always easy.
- Instead of: “That much plaque usually means you haven’t been brushing properly.”
- Try: “I’m noticing some plaque build-up. It’s very common. A lot of my patients are surprised by how much even small changes in brushing habits can make a difference. Do you mind if I share some tips?”
This approach validates the patient’s experience, making them more likely to open up and engage.

3. Look to the future, not the past
While it is important to understand the patient’s habits, avoid lingering on what they have done “wrong.” Instead, focus on what can be done moving forward. This encourages a growth mindset and reduces the risk of a shame-based shutdown.
- Instead of: “If you had come in sooner, we could have avoided this.”
- Try: “It is good that you came in today, so we could get this sorted out. Now, let’s talk about the steps you can take to support the healing process.”
By framing the conversation around the steps the patient can take going forward, it becomes hopeful instead of judgmental.

4. Focus on positive outcomes, not negative consequences
Long-term behavioural change is most successful when people feel safe, respected, and supported. In other words, when they believe they are capable of improvement, not that they have already failed. So while it might be tempting to highlight risks of tooth decay, gum disease, or the need for expensive treatments down the line, it is more effective to focus on the positives, like fresh breath, less discomfort, fewer appointments, and better long-term health.
- Instead of: “You will lose that tooth if you don’t start brushing better.”
- Try: “If you keep up with this technique, you will give that tooth the best chance to stay healthy.”
This way you invite the patient to see themselves as capable of change, not guilty of neglect.
5. Invite collaboration, not compliance
When the patient actively participates in the conversation, your advice will not feel like a lecture, but rather something you have agreed upon together. Use language that encourages partnership rather than passive obedience:
- Instead of: “You need to start using interdental brushes.”
- Try: “Would you be open to trying something that can make it easier to clean between your teeth?”
This kind of collaborative tone shifts the dynamic away from shame and judgment toward shared responsibility.
Want to provide better support for patients struggling with difficult emotions?
Managing shame during conversations about oral health habits is a great place to start, but it is not the only time this challenging emotion can show up during a dental appointment.
We have designed the very first human-first dentistry course for dental professionals who want to strengthen their soft skills to provide better support for patients struggling with difficult emotions like shame and anxiety. This course is led by anxiety specialist and best-selling author Denisa Moravcik Debrecka and helps you to:
- Easily spot signs your patient is experiencing emotional distress.
- Learn the common and less common triggers in your practice.
- React to any patient interaction with empathy and validation.
- Improve the patient experience from pre-appointment to post-procedure with an actionable step-by-step guide.
Sources
- Talker Research surveyed 2,000 general population Americans in 2025; the survey was commissioned by Aspen Dental.
- Doughty J, Macdonald ME, Muirhead V, Freeman R. Oral health-related stigma: Describing and defining a ubiquitous phenomenon. Community Dent Oral Epidemiol. 2023; 51: 1078-1083.
- Dolezal L, Lyons B Health-related shame: an affective determinant of health? Medical Humanities 2017; 43:257-263.
- Yuan S, Freeman R, Hill K, Newton T, Humphris G. Communication, Trust and Dental Anxiety: A Person-Centred Approach for Dental Attendance Behaviours. Dentistry Journal. 2020; 8(4):118.